
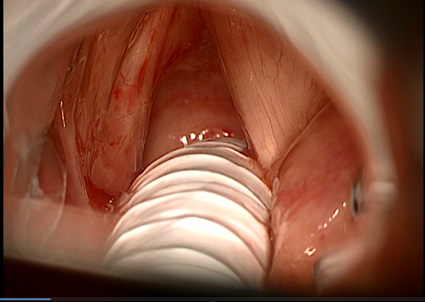
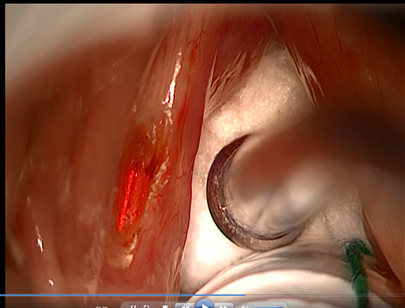
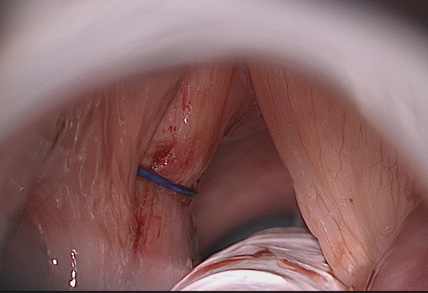
These are 4 consecutive steps of the laterofixation procedure. After vocal muscle submucosal vaporization by CO2 Acublade laser, vocal fold lateralization is achieved by a single endo-extralaryngeal stitch.
LATEROFIXATION AS A MINI-INVASIVE TREATMENT TO RELEIVE RESPIRATORY OBSTRUCTION IN BILATERAL LARYNGEAL PARALYSIS

The paralysis of both vocal folds is an uncommon condition that can cause severe chronic respiratory obstruction due to a reduction of the laryngeal respiratory space.
The paralyzed vocal folds are not any more able to abduct (=to open) to let air flow to the lungs in inspiration. This condition can become critical during efforts or when the larynx is inflamed due to upper airway infection. Swallowing efficiency and voice quality can also be impaired, but the respiratory problem is usually the most critical one.
Several techniques have been proposed over the years to widen the respiratory space, they include either tissue ablation or tissue displacement. The latter can be more physiological and can minimize the consequences of surgery.
The main problems encountered after surgery for a bilateral vocal fold paralysis are worsening of voice and of swallowing efficiency.
I have adopted the technique described in the past by professor Lichtenberger in Hungary modifying it in a mini-invasive version. Instead of taking out part of one vocal fold, the treated fold is fixed with a stitch in a more lateral position to widen the respiratory space. Before passing the stitch we make a submucosal partial resection of the adductor muscle in order to create a scar that will help keeping the vocal fold in open position.
This technique does not cause swallowing impairment and causes moderate or mild voice changes.
