
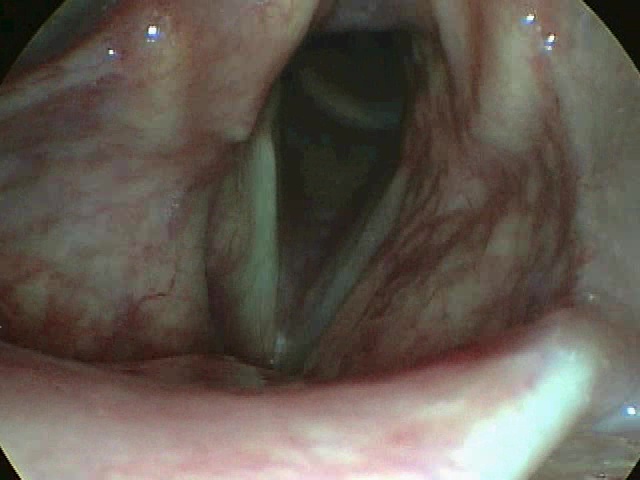
Paralysis of the right vocal fold consequent to thyroidectomy
AUTOLOGOUS FAT INJECTION FOR VOICE IMPROVEMENT IN UNILATERAL PARALYSES OF THE VOCAL FOLDS


The patient has a breathy voice as the vocal folds do not get in contact during phonation
Four years after fat grafting to the right vocal fold; view during inspiration

Four years after fat grafting the vocal folds can close during phonation. The patient has a normal voice.
Vocal fold paralyses are mainly due to a peripheral lesion of the recurrent laryngeal nerve, which provides innervation to the intrinsic muscles of the larynx (known as voice box). A lesion of this nerve severely impairs the movement of the involved vocal fold. The lesion can be due to several causes such as compression and infiltration by neck masses, but the most common causes are accidental lesions during surgery on the neck or chest; sometimes the cause of the paralysis remains unknown and might probably be the consequence of viral infection.
The side most often involved is the left one due to the long and complex route of the left recurrent nerve . Injury to the nerve results in a weakened, breathy voice. The effort required by voice production can be so relevant to cause general fatigue due to the respiratory strain necessary to sustain the voice. The patient can experience also a swallowing impairment while respiratory obstructive symptoms are most commonly present only if both nerves are injured. Voice therapy is the first line treatment but, if it does not give a satisfying result or if there is a professional and social necessity to regain promptly an efficient voice, then a mini-invasive surgical procedure such as autologous fat injection can achieve a fast and definitive result.
Injection augmentation of the paralyzed vocal fold improves vocal fold closure during voice production, and corrects the flaccidity of the atrophic vocal fold allowing recovery of its vibration in synchrony with the contralateral moving fold.
Over the years several materials have been employed to achieve vocal fold augmentation; non-reabsorbable implants such as silicone or its derivatives can migrate or give raise to foreign body inflammatory reactions; the reabsorbable materials such as collagen and hyaluronic acid do not provide a permanent result.
Since more than 15 years I perform the vocal fold fat augmentation procedure applying the principles described by Sidney Coleman for esthetic and reconstructive surgery. The fat is taken from the abdomen mini-invasively by liposuction, it is processed and the obtained purified fat parcels are injected in the vocal folds trans-orally under direct microscopic vision. The voice improvement is usually very fast and a reduction in voice fatigue is immediately perceived by the patient.
Several international studies have demonstrated that the regenerative potential of fat injection is mediated by its content in stem cells and growth factors. Therefore this type of operation can be defined a regenerative approach.
